When Should You Get Screened for Prostate Cancer? Essential Clinical Guidelines for Prostate Health
Why Is Early Prostate Cancer Screening Crucial for Men in Cheonan?
Prostate cancer is one of the most common malignancies in men, characterized by its slow progression and lack of early-stage symptoms. The prostate is a walnut-sized gland located below the bladder, wrapping around the urethra. Prostate cancer arises from the malignant transformation of epithelial cells in this gland, a progressive condition that can eventually metastasize to bones and lymph nodes if left undetected. Because early-stage prostate cancer rarely causes noticeable urinary issues, routine screening is the primary mechanism for timely intervention. In the target region of Cheonan, access to specialized urology departments allows patients to undergo precise screening protocols before advanced symptoms manifest.
Treatment timing: Annual screening should begin at age 50 for average-risk men, or age 40 for individuals with a first-degree relative diagnosed with prostate cancer.
Non-surgical care: Conservative management, such as active surveillance or watchful waiting, is highly reasonable for low-risk, localized prostate cancers with low Gleason scores and stable PSA kinetics.
Treatment selection: Treatment decisions are determined by tumor stage, histological aggressiveness, age, overall health status, and patient preference regarding quality-of-life trade-offs.

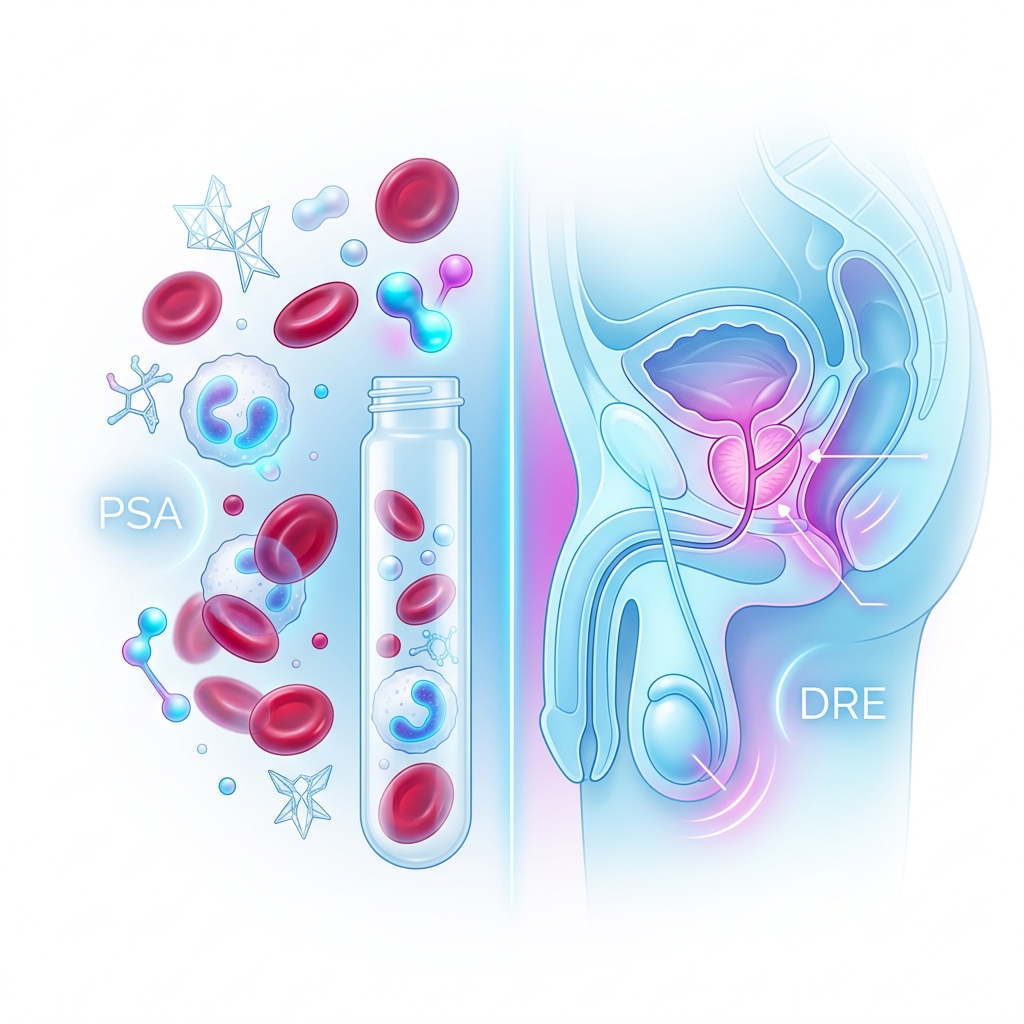
How Do PSA Testing and Digital Rectal Exams Compare in Diagnostic Accuracy?
According to multiple observational studies and meta-analyses, combining different screening modalities significantly increases the detection rate of clinically significant prostate cancer. While the Prostate-Specific Antigen (PSA) blood test is highly sensitive, it can be elevated by non-cancerous conditions such as benign prostatic hyperplasia (BPH) or prostatitis. Therefore, a physical evaluation remains essential. The Digital Rectal Exam (DRE) allows a urologist to palpate the posterior surface of the prostate gland to detect physical abnormalities such as nodules, asymmetry, or hard induration that a blood test alone might miss.
| Screening Method | Primary Clinical Advantage | Diagnostic Limitation |
|---|---|---|
| PSA Blood Test | Highly sensitive, minimally invasive blood draw tracking systemic biomarkers. | High false-positive rate due to benign prostatic hyperplasia or inflammation. |
| Digital Rectal Exam (DRE) | Direct physical assessment of prostate size, consistency, and structural nodules. | Highly subjective, dependent on examiner skill, and misses anterior tumors. |
| Multiparametric MRI (mpMRI) | Excellent anatomical and functional visualization for targeting biopsies. | Requires specialized imaging hardware and is not used as a primary screening tool. |
According to official guidelines from international urological associations, both quantitative PSA velocity criteria and clinical physical findings should be reviewed together to determine the necessity of a prostate biopsy.
What Is the Diagnostic Protocol for Elevated PSA Levels?
When a screening test reveals an elevated PSA level (typically above 3.0 or 4.0 ng/mL, depending on age guidelines), immediate biopsy is not always the first step. Clinical guidelines emphasize a structured, sequential approach to rule out temporary confounding factors and confirm true oncological risk. For patients presenting at a urology department in Cheonan, urologists utilize localized diagnostic algorithms to minimize unnecessary anxiety and invasive procedures.
- Step 1: Repeat PSA Test: Confirm the elevation with a second blood test after avoiding strenuous exercise, sexual activity, or urinary tract instrumentation.
- Step 2: Assess Free-to-Total PSA Ratio: Evaluate the percentage of free PSA, which is often lower in malignant cases compared to benign conditions.
- Step 3: Multiparametric MRI: Perform high-resolution imaging to localize suspicious lesions and assign a PI-RADS score.
- Step 4: Targeted Prostate Biopsy: Execute a systematic or fusion biopsy under ultrasound guidance to obtain tissue samples for histological analysis.
- Step 5: Gleason Scoring: Analyze biopsy tissues to grade the aggressiveness of the cells, directing the subsequent management pathway.
However, outcomes may differ in exceptional cases such as very elderly patients with significant comorbidities, where active treatment may not prolong life expectancy, and conservative watchful waiting is preferred regardless of biopsy grading.
Clinical Decision-Making Flow:
IF PSA level is between 3.0 and 10.0 ng/mL with no physical nodules, THEN perform a free/total PSA ratio test and repeat PSA evaluation in 4-6 weeks.
IF the free PSA ratio is below 15% or PSA continues to rise, THEN proceed to a multiparametric MRI (mpMRI).
IF the MRI reveals a PI-RADS score of 3 or higher, THEN recommend a targeted prostate biopsy.
Frequently Asked Questions FAQ
QDoes a high PSA level always mean I have prostate cancer?
No. A high Prostate-Specific Antigen (PSA) level can be caused by benign conditions such as benign prostatic hyperplasia (BPH), acute or chronic prostatitis, recent urinary tract infections, or physical trauma to the pelvic region. A comprehensive evaluation by a urologist is necessary to determine the exact cause of the elevation.
QHow painful is a prostate biopsy, and how long is the recovery?
A prostate biopsy is performed under local anesthesia or sedation, making discomfort highly manageable. The procedure typically takes 15 to 20 minutes. Patients may experience minor soreness, light rectal bleeding, or blood in the urine or semen for a few days to weeks. Normal light activities can usually be resumed within 24 to 48 hours.
QCan lifestyle modifications help prevent prostate cancer?
While lifestyle changes cannot guarantee prevention, clinical evidence suggests that a diet rich in lycopene (found in cooked tomatoes), cruciferous vegetables, and healthy fats, combined with regular physical exercise and weight management, plays a supportive role in reducing the risk of aggressive prostate cancer progression.

This content is general medical information, and individual treatment decisions should be made through imaging tests and in-person medical evaluation.
Author: Medical content editor based on medical information research
Reviewed by: Specialist consultation from the relevant department
Last reviewed: 2026-06-29
Reference guideline: 2024 European Association of Urology (EAU) Guidelines on Prostate Cancer
Medical neutrality and closing note
The core of medical decision-making is not to follow a specific device or a trending procedure, but to choose an option that fits each patient’s individual anatomy, condition, risk level, and treatment goals. Every procedure has both advantages and limitations, so decisions should be made after sufficient discussion with an experienced specialist.
[Medical information and copyright notice]
This content is a professional medical column prepared based on medical consultation from 굿모닝비뇨기과.
The infographics used in this article are created to support understanding and may differ from actual clinical results.
The information provided is a general medical guideline, and accurate diagnosis and treatment require an in-person evaluation by a qualified specialist.