1. Medically, urolithiasis is defined as the formation of crystalline mineral deposits within the renal pelvis or ureter, often presenting with paroxysmal renal colic and microscopic hematuria.
2. Conservative management is reasonable when stones are <5mm in diameter, asymptomatic, and located in a position likely to pass spontaneously without causing high-grade hydronephrosis.
3. Choosing a diagnostic center requires verifying the availability of non-contrast CT protocols, real-time Doppler ultrasound, and dedicated international patient coordination to manage recovery timelines.

Comparative Analysis of Primary Diagnostic Modalities
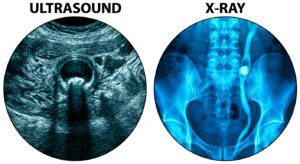
The initial evaluation of a male patient suspected of having urinary stones typically begins with a combination of laboratory tests and imaging. While non-contrast computed tomography (NCCT) is widely considered the gold standard for sensitivity, the role of ultrasound remains pivotal, especially for monitoring and for patients seeking to minimize radiation exposure. International medical society guidelines indicate that the sensitivity of ultrasound for detecting renal stones ranges from 45% to 80%, depending on stone size and the patient’s body mass index (2022–2024 aggregate data). In the medical district, many facilities utilize advanced Doppler-enhanced ultrasound to improve the detection of the ‘twinkling artifact,’ a phenomenon that assists in identifying small stones that might be missed by conventional B-mode imaging.
However, in exceptional cases where the stone is located in the mid-ureter and obscured by bowel gas, the diagnostic yield of ultrasound may significantly decrease.
| Diagnostic Criteria | High-Resolution Ultrasound | Non-Contrast CT (NCCT) |
|---|---|---|
| Primary Advantage | Zero radiation; real-time hydronephrosis assessment | Highest sensitivity (95%+) for all stone sizes |
| Anatomic Coverage | Excellent for kidney/bladder; limited for mid-ureter | Full urinary tract visualization from kidney to urethra |
| Typical Duration | 15–20 minutes | 5–10 minutes |
| Recovery/Downtime | Immediate return to travel activities | Immediate; requires consideration of radiation cumulative dose |
Multiple peer-reviewed publications report that for international travelers, the speed of diagnosis is a critical factor in determining the length of stay. Clinical data from specialized centers suggests that a streamlined ‘one-stop’ system—integrating urinalysis, ultrasound, and specialist consultation within 2 hours—significantly reduces patient anxiety and facilitates faster intervention if required.
However, in exceptional cases where patients have pre-existing renal insufficiency, the use of contrast-enhanced imaging must be strictly avoided to prevent contrast-induced nephropathy.
The Role of Urinalysis in Differential Diagnosis
The pathophysiology of urinary stones involves the supersaturation of urine with salts such as calcium oxalate, uric acid, or cystine. According to multiple observational studies and meta-analyses, approximately 85% of patients with acute urinary stones present with microscopic hematuria, which is the presence of red blood cells in the urine. This laboratory screen serves as a vital ‘red flag’ that distinguishes renal colic from other types of abdominal pain, such as appendicitis or musculoskeletal strain. Beyond detecting blood, this diagnostic screen measures urinary pH; a low pH (acidic) may suggest uric acid stones, while a high pH (alkaline) might indicate an infection-related struvite stone.
International medical society guidelines indicate that the presence of nitrites or leukocyte esterase during a laboratory analysis of the specimen warrants immediate investigation for a concomitant urinary tract infection (UTI). A stone combined with an infection is a medical emergency that requires prompt drainage, often through a ureteral stent or nephrostomy tube, before definitive stone fragmentation is attempted.
However, in exceptional cases where a stone is completely obstructing the ureter, the urinalysis may paradoxically appear normal because no urine from the affected kidney is reaching the bladder.
Selection Criteria for International Patients: A Checklist
When seeking urological care abroad, international patients should look for institutions that prioritize evidence-based protocols and patient safety. Clinical data from specialized clinics suggests that successful outcomes are highly correlated with the technology used for diagnosis and the experience of the urologist in performing minimally invasive procedures like Extracorporeal Shockwave Lithotripsy (ESWL) or Ureteroscopy (URS).
- Specialized Imaging Technology: Does the medical institution utilize high-definition ultrasound and low-dose CT protocols to minimize radiation while maintaining diagnostic clarity?
- Immediate Intervention Capability: If a stone is found to be 7mm or larger, can the facility provide ESWL or laser lithotripsy on the same day or the following day?
- International Support Services: Is there an English-speaking coordinator available to explain the results of the aforementioned procedure and assist with insurance documentation?
- Integrated Laboratory Services: Are urine and blood results processed on-site to ensure a rapid turnaround time for patients with limited travel schedules?
- Post-Procedure Follow-up: Does the facility provide a detailed medical report and digital imaging copies for your home-country physician to ensure continuity of care?
However, in exceptional cases where the patient has a high-risk cardiac profile, certain leading providers may require additional cardiovascular clearance before proceeding with even minor sedated procedures.
Decision-Making Flow for Acute Urinary Symptoms
For patients navigating this process, the following logic helps determine the next medical steps:
- Step 1: If sudden flank pain is accompanied by fever or chills → Then: Seek immediate emergency evaluation for possible obstructive pyelonephritis.
- Step 2: If urinalysis confirms microscopic hematuria and ultrasound shows >5mm stone → Then: Compare the benefits of ESWL versus conservative medical expulsive therapy (MET) based on stone location.
- Step 3: If the patient is an international traveler with a flight scheduled within 48 hours → Then: Prioritize definitive treatment (lithotripsy) over conservative management to avoid a pain crisis during travel.
However, in exceptional cases where the stone is asymptomatic and non-obstructive, a ‘wait-and-see’ approach may be medically reasonable provided there is a plan for follow-up in the patient’s home country.
Frequently Asked Questions for Medical Tourists
A: For diagnostic evaluation and non-surgical treatment like ESWL, a stay of 3 to 5 days is typically sufficient. This allows time for the initial procedure and a follow-up ultrasound to confirm stone fragmentation and ensure no complications arise before your flight.
A: Yes, many premier facilities in major medical districts employ board-certified urologists who are proficient in English and provide dedicated international desks to manage the needs of foreign patients.
A: While ultrasound has no travel restrictions, after a fragmentation procedure, most urologists suggest waiting 24 to 48 hours. This ensures that any initial hematuria or ‘steinstrasse’ (a buildup of stone fragments in the ureter) is managed while you are still near the medical institution.
A: Many providers offer remote consultations where you can share your home-country laboratory results and imaging. This allows the local medical community to prepare a treatment plan before you even arrive, maximizing the efficiency of your visit.

This content represents general medical information, and individual treatment decisions should be made through imaging diagnostics and in-person consultation with a qualified medical professional.
Medical Review: Specialist in Urology
Last Reviewed: {TODAY_DATE}
Reference Guidelines: European Association of Urology (EAU) Guidelines on Urolithiasis (2023), American Urological Association (AUA) Kidney Stone Guidelines.
Medical Neutrality and Closing Notes
The essence of this treatment lies not in following a specific device or trending technique, but in making the medical choice most suited to each patient’s individual anatomy and condition. Every procedure has both advantages and limitations, and thorough consultation with a qualified specialist is essential before any decision.
[Medical Information Disclosure and Copyright Notice]
• This content has been produced as a professional medical column based on the medical advisory of 굿모닝비뇨기과, a medical institution located in South Korea.
• Infographics used in this article were created with the assistance of AI technology for illustrative purposes and may differ from actual clinical outcomes.
• The information provided reflects general medical guidelines. For accurate diagnosis and treatment, please visit a qualified medical institution and consult directly with a specialist.
• For inquiries regarding English-language consultation, international patient services, or medical travel arrangements, please contact the medical institution directly.
This content is provided for general medical information purposes, and individual diagnostic and treatment decisions should be made through consultation with qualified medical professionals.