How to Choose the Safest Endoscopic Stone Surgery: Criteria, 9 Advanced Systems, and Recovery Guidelines
Why is Precise Diagnosis Critical for Urinary Stones?
Urinary stone disease, or urolithiasis, is a progressive condition characterized by the crystallization of mineral salts within the urinary tract, which can cause acute obstructive uropathy, severe renal colic, and progressive renal dysfunction if left untreated. Choosing the correct intervention requires assessing stone size, density, and location. According to multiple observational studies and meta-analyses, specifically the European Association of Urology (EAU) Guidelines (2023), stones exceeding 10mm or those failing conservative management require active intervention to prevent long-term renal damage.
Treatment timing: Active intervention is indicated when urinary stones exceed 10mm, cause intractable pain, or induce progressive hydronephrosis.
Non-surgical care: Conservative management, including hydration and medical expulsive therapy, is reasonable primarily for asymptomatic stones under 5mm without signs of urinary tract infection or complete obstruction.
Treatment selection: The choice between shockwave lithotripsy and endoscopic surgery is guided by stone density (measured in Hounsfield units), anatomical complexity, and individual patient risk levels.

What are the Key Differences Between Non-Invasive and Endoscopic Treatments?
When selecting a treatment modality, clinicians balance the efficacy and invasiveness of each option. Retrograde Intrarenal Surgery (RIRS) and Extracorporeal Shockwave Lithotripsy (ESWL) are the primary options. RIRS provides a major advantage of achieving a high stone-free rate in a single session even for hard, complex stones; however, its primary limitation is the requirement for general anesthesia and temporary ureteral stenting. Conversely, ESWL is non-invasive and performed without anesthesia, but has a lower success rate for stones with high density or those located in the lower renal pole.
| Treatment Option | Primary Advantage | Key Limitation | Indications |
|---|---|---|---|
| Retrograde Intrarenal Surgery (RIRS) | High stone-free rate for hard/multiple stones | Requires general anesthesia and stenting | Stones >10mm, lower pole stones, failed ESWL |
| Extracorporeal Shockwave Lithotripsy (ESWL) | Outpatient procedure, no anesthesia required | Lower success rate for hard stones (>1000 HU) | Soft stones <10mm, uncomplicated cases |
According to official guidelines or academic evidence, both quantitative criteria and clinical judgment should be reviewed together.
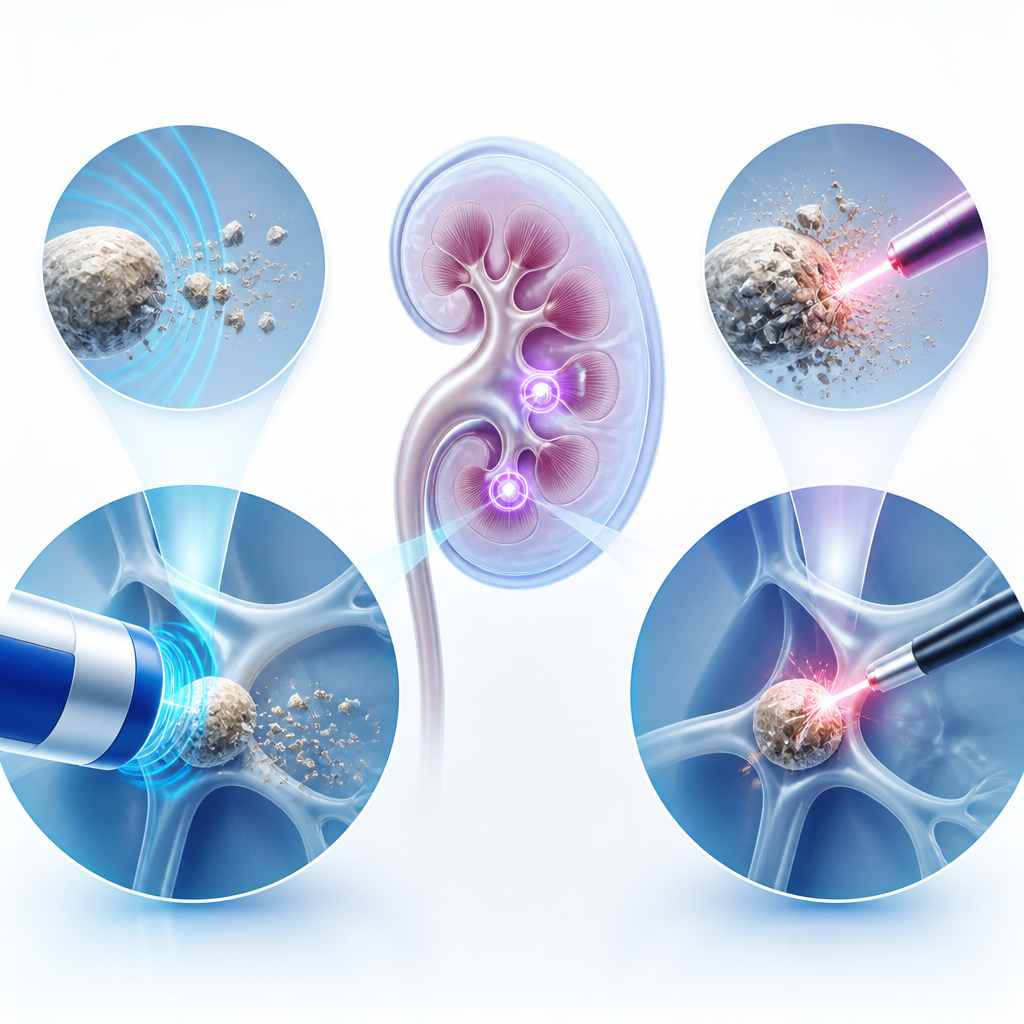
How Do 9 Advanced Endoscopic Systems Enhance Patient Safety?
Modern urological interventions rely heavily on specialized technology. Utilizing a diverse suite of 9 advanced endoscopic stone surgery systems allows for highly customized procedures tailored to the patient’s unique anatomy. These systems incorporate ultra-thin, flexible ureteroscopes and high-power holmium laser fibers that can navigate the delicate contours of the kidney without causing mucosal tearing. However, outcomes may differ in exceptional cases such as severe anatomical anomalies of the urinary tract or uncorrected bleeding diathesis.
- Anatomical Mapping: High-definition visualization systems provide real-time, 4K resolution of the renal pelvis to locate hidden stone fragments.
- Minimized Tissue Trauma: Flexible ureteroscopes with small outer diameters reduce the risk of ureteral stricture or perforation.
- Efficient Dusting: Advanced holmium and thulium laser technologies allow for “dusting” of stones, reducing the need for basket extraction.
- Intraocular Pressure Control: Specialized irrigation systems maintain safe fluid pressure within the kidney during the procedure.
To assist in the clinical decision-making process, patients and clinicians can follow this simple mini-flow:
Evaluate Stone Density: If stone density exceeds 1,000 Hounsfield Units, prioritize endoscopic laser lithotripsy over shockwave therapy.
Assess Size & Location: If the stone is located in the lower pole and is larger than 10mm, proceed directly to RIRS.
Confirm Clinical Status: If signs of active infection or severe hydronephrosis are present, perform immediate decompression followed by staged endoscopic clearance.
Frequently Asked Questions FAQ
QIs endoscopic stone surgery painful during and after the procedure?
The procedure itself is performed under general or regional anesthesia, meaning there is no pain during the surgery. After the procedure, mild discomfort, hematuria, or bladder spasms may occur due to the temporary ureteral stent, but these symptoms are typically manageable with oral medication and subside within a few days.
QWhat is the average recovery time before returning to normal activities?
Most patients can return to light daily activities within 24 to 48 hours after retrograde intrarenal surgery (RIRS). Strenuous exercise should be avoided until the temporary ureteral stent is removed, which typically occurs 1 to 2 weeks post-procedure.
QWhy are multiple advanced endoscopic systems important for safety?
Having access to a wide range of specialized equipment, such as 9 distinct endoscopic systems, allows the surgeon to select the precise scope size and laser frequency that matches the patient’s specific anatomy and stone composition, thereby minimizing potential complications.
This content is general medical information, and individual treatment decisions should be made through imaging tests and in-person medical evaluation.
Author: Medical content editor based on medical information research
Reviewed by: Specialist consultation from the relevant department
Last reviewed: 2026-06-18
Reference guideline: 2023 European Association of Urology (EAU) Guidelines on Urolithiasis
Medical neutrality and closing note
The core of medical decision-making is not to follow a specific device or a trending procedure, but to choose an option that fits each patient’s individual anatomy, condition, risk level, and treatment goals. Every procedure has both advantages and limitations, so decisions should be made after sufficient discussion with an experienced specialist.
[Medical information and copyright notice]
This content is a professional medical column prepared based on medical consultation from 굿모닝비뇨기과.
The infographics used in this article are created to support understanding and may differ from actual clinical results.
The information provided is a general medical guideline, and accurate diagnosis and treatment require an in-person evaluation by a qualified specialist.