When Should You Seek Emergency Urinary Tract Stone Treatment in Ssangyong-dong? Key Symptoms and Decision Criteria
Are You Experiencing Sudden, Agonizing Pain in Your Lower Back or Abdomen in Ssangyong-dong?
An acute episode of urinary tract stones is often described as one of the most intense physical pains a person can experience. When a crystalline mineral mass blocks the narrow ureter, the body reacts with sharp, spasmodic contractions to push the blockage through. For residents experiencing these severe symptoms in Ssangyong-dong, knowing whether to wait for spontaneous passage or seek immediate care at a specialized urology clinic is vital to avoiding severe kidney damage and systemic infection.
A urinary tract stone (urolithiasis) is a progressive mineral deposition disease where crystalline aggregates form in the renal pelvis and migrate through the ureter, causing acute, severe flank pain, microscopic hematuria, and potentially obstructive uropathy if left untreated. It is an active, progressive process; as the stone remains lodged, the pressure within the renal pelvis escalates, leading to hydronephrosis and a gradual decline in renal function. Early diagnostic evaluation through low-dose computed tomography (CT) or ultrasonography is key to identifying the precise size, density, and location of the stone.
Treatment timing: Urgent intervention is required if the stone is larger than 5 mm, accompanied by fever, or causing complete urinary tract obstruction and intractable pain.
Non-surgical care: Conservative management using medical expulsive therapy (such as alpha-blockers) and hyper-hydration is appropriate only for uncomplicated stones smaller than 5 mm.
Treatment selection: The choice between non-invasive extracorporeal shock wave lithotripsy (ESWL) and minimally invasive ureteroscopy (URS) depends on stone size, location, and the presence of renal obstruction.

How Do Treatment Options Compare for Different Stone Sizes and Locations?
Clinical decision-making in urology is highly standardized based on the physical dimensions and anatomical location of the calculus. According to multiple clinical guidelines, stones measuring under 5 mm have a high probability of passing spontaneously without active intervention, provided there is no sign of renal impairment. However, once a stone exceeds this threshold or becomes impacted, advanced urological treatments must be considered.
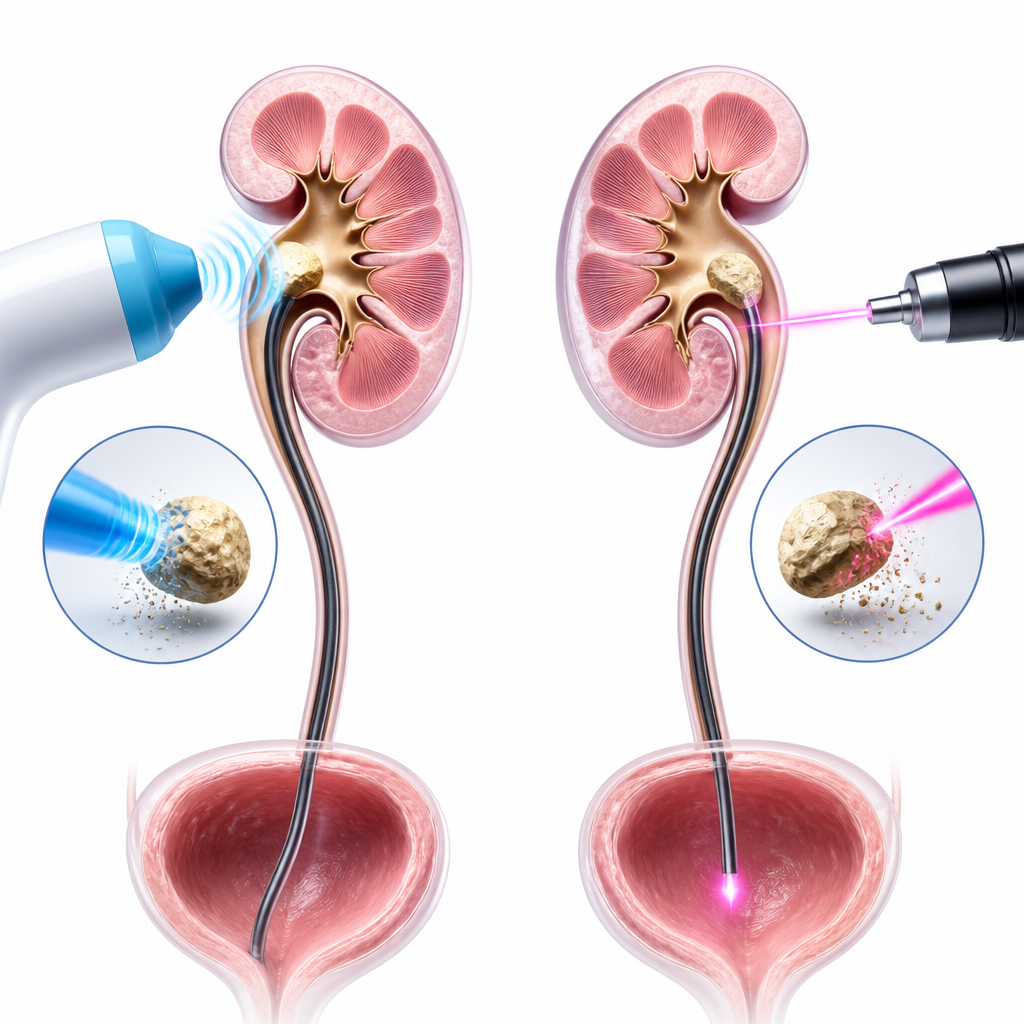
The two primary active interventions are Extracorporeal Shock Wave Lithotripsy (ESWL) and Ureteroscopy (URS). ESWL is a non-invasive outpatient procedure that uses targeted acoustic shock waves to fragment the stone into sand-like particles. URS is a minimally invasive endoscopic procedure performed under anesthesia, where a thin scope is passed through the urethra to directly fragment the stone using a laser holmium fiber and retrieve the fragments with a basket.
| Treatment Type | Primary Advantage | Key Limitation | Typical Indication |
|---|---|---|---|
| Conservative Expulsive Therapy | No procedural risks or recovery time | Unpredictable duration and risk of sudden pain recurrence | Stones < 5 mm without complications |
| Shock Wave Lithotripsy (ESWL) | Non-invasive, no anesthesia, outpatient setting | Lower success rate for hard or large stones (> 15 mm) | Uncomplicated renal or upper ureteral stones |
| Ureteroscopy (URS) | Immediate, near 100% stone-free rate in a single session | Requires anesthesia and temporary double-J stent placement | Lower ureteral stones, hard stones, or ESWL failures |
According to official guidelines from the European Association of Urology (EAU) 2021, while spontaneous passage is highly expected for small ureteral calculi, active treatment should not be delayed beyond 4 to 6 weeks if the stone remains stationary, as prolonged obstruction significantly increases the risk of permanent renal parenchymal loss.
What Clinical Checklist Helps Determine the Urgency of Stone Treatment?
For patients suffering from suspected urinary tract stones in Ssangyong-dong, evaluating the severity of the clinical presentation is critical. The following clinical checklist helps identify whether conservative monitoring is safe or if immediate specialist care at a urology clinic is required:
- Severity of Pain: Is the flank or groin pain manageable with oral over-the-counter analgesics, or is it intractable and causing vomiting?
- Presence of Fever: Do you have a body temperature above 38°C (100.4°F) accompanied by chills? (This is a medical emergency indicating obstructive pyelonephritis).
- Urinary Output: Are you experiencing a noticeable reduction in urine volume, or an inability to void despite a strong urge?
- Stone Size and Location: Has a diagnostic ultrasound or CT scan confirmed a stone size larger than 5 to 6 mm?
- Duration of Symptoms: Have you been experiencing continuous or intermittent colic symptoms for more than 4 weeks without stone passage?
Based on these parameters, clinicians utilize an If-Then Decision Framework to guide patient care:
Step 1: If the stone is < 5 mm and pain is manageable without signs of infection, Then initiate medical expulsive therapy with alpha-blockers, encourage a daily fluid intake of over 2.5 liters, and monitor via weekly imaging.
Step 2: If the stone is > 6 mm, or if conservative therapy fails to dislodge the stone within 4 weeks, Then schedule active intervention such as ESWL or ureteroscopic lithotripsy to prevent long-term ureteral scarring.
Step 3: If there is concurrent fever, chills, anuria, or acute kidney injury (AKI) markers, Then perform urgent decompression via retrograde ureteral stenting or percutaneous nephrostomy prior to definitive stone fragmentation.
However, outcomes may differ in exceptional cases such as patients with a solitary kidney, pre-existing chronic kidney disease, or pregnant patients, where traditional treatment protocols must be highly customized to protect both maternal and fetal health.
Frequently Asked Questions FAQ
QIs it possible for a urinary tract stone to dissolve naturally with medication?
Generally, only uric acid stones, which account for approximately 10% of all cases, can be dissolved medically using oral chemolysis with alkalinizing agents like potassium citrate. The vast majority of stones are composed of calcium oxalate or calcium phosphate, which cannot be dissolved by drinking water or taking medication, and must be passed spontaneously or fragmented actively.
QHow long does recovery take after undergoing ESWL or ureteroscopic surgery?
Recovery after non-invasive ESWL is immediate; most patients return to normal daily activities within 24 hours, though they may experience mild hematuria and passing of stone fragments for several days. After ureteroscopic surgery (URS), recovery takes about 2 to 3 days, and some discomfort or urinary urgency may persist until the internal double-J ureteral stent is removed, typically within 1 to 2 weeks.
QWhat are the best preventive steps to avoid a recurrence of urinary tract stones in Ssangyong-dong?
Because the recurrence rate of urolithiasis is nearly 50% within five years, prevention is essential. Residents in Ssangyong-dong should maintain a daily fluid intake sufficient to produce 2 to 2.5 liters of clear urine, reduce dietary sodium and animal protein intake, and avoid excessive oxalate-rich foods while maintaining a normal dietary calcium intake.

This content is general medical information, and individual treatment decisions should be made through imaging tests and in-person medical evaluation.
Author: Medical content editor based on medical information research
Reviewed by: Specialist consultation from the relevant department
Last reviewed: 2026-06-19
Reference guideline: 2021 European Association of Urology (EAU) Urolithiasis Guidelines
Medical neutrality and closing note
The core of medical decision-making is not to follow a specific device or a trending procedure, but to choose an option that fits each patient’s individual anatomy, condition, risk level, and treatment goals. Every procedure has both advantages and limitations, so decisions should be made after sufficient discussion with an experienced specialist.
[Medical information and copyright notice]
This content is a professional medical column prepared based on medical consultation from 굿모닝비뇨기과.
The infographics used in this article are created to support understanding and may differ from actual clinical results.
The information provided is a general medical guideline, and accurate diagnosis and treatment require an in-person evaluation by a qualified specialist.