What Are the Crucial Signs of Bladder Cancer, and When Should You Visit a Urology Clinic in Ssangyong-dong?
Why Is Early Detection the Ultimate Factor in Overcoming Bladder Cancer?
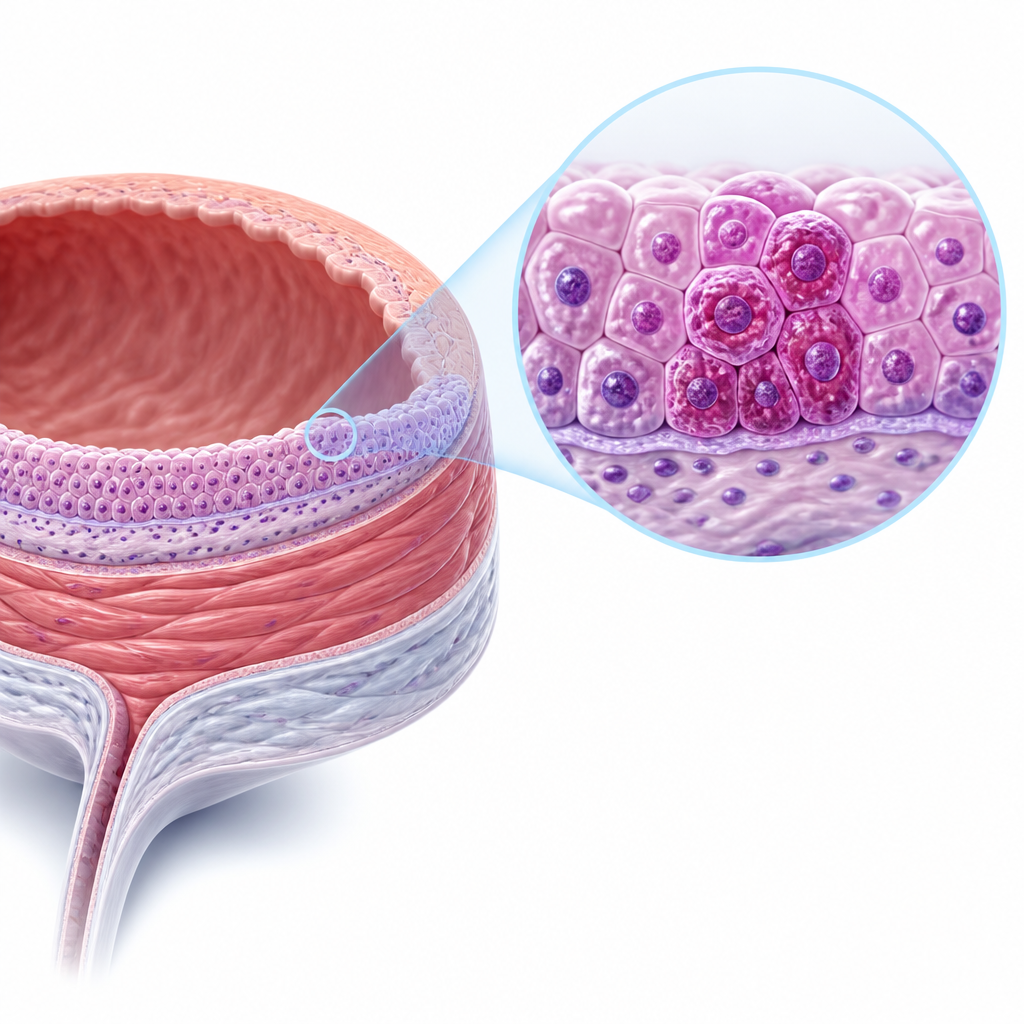
Bladder cancer is a progressive oncological disease originating primarily in the urothelium—the transitional epithelial lining of the urinary bladder. Anatomically, it begins as a superficial lesion but possesses a high propensity to invade the deeper detrusor muscle layer if left untreated. According to clinical data published by the National Cancer Center in 2023, early-stage bladder cancer (Non-Muscle-Invasive Bladder Cancer, or NMIBC) has a high survival rate, whereas muscle-invasive stages present a significantly poorer prognosis. Patients in Ssangyong-dong experiencing unexplained changes in urination must understand the pathophysiological progression of this disease to seek timely help at a local urology clinic.
Treatment timing: Diagnostic evaluation must begin within 2 to 4 weeks of experiencing painless hematuria to prevent the progression of superficial tumors to invasive stages.
Non-surgical care: Conservative management, such as intravesical BCG immunotherapy or chemotherapeutic instillations, is highly reasonable for low-to-intermediate risk non-muscle-invasive bladder cancer following initial resection.
Treatment selection: Therapeutic choices are guided by the depth of tumor invasion (T stage), histological grading (low vs. high grade), and the patient’s overall renal function and recovery expectations.
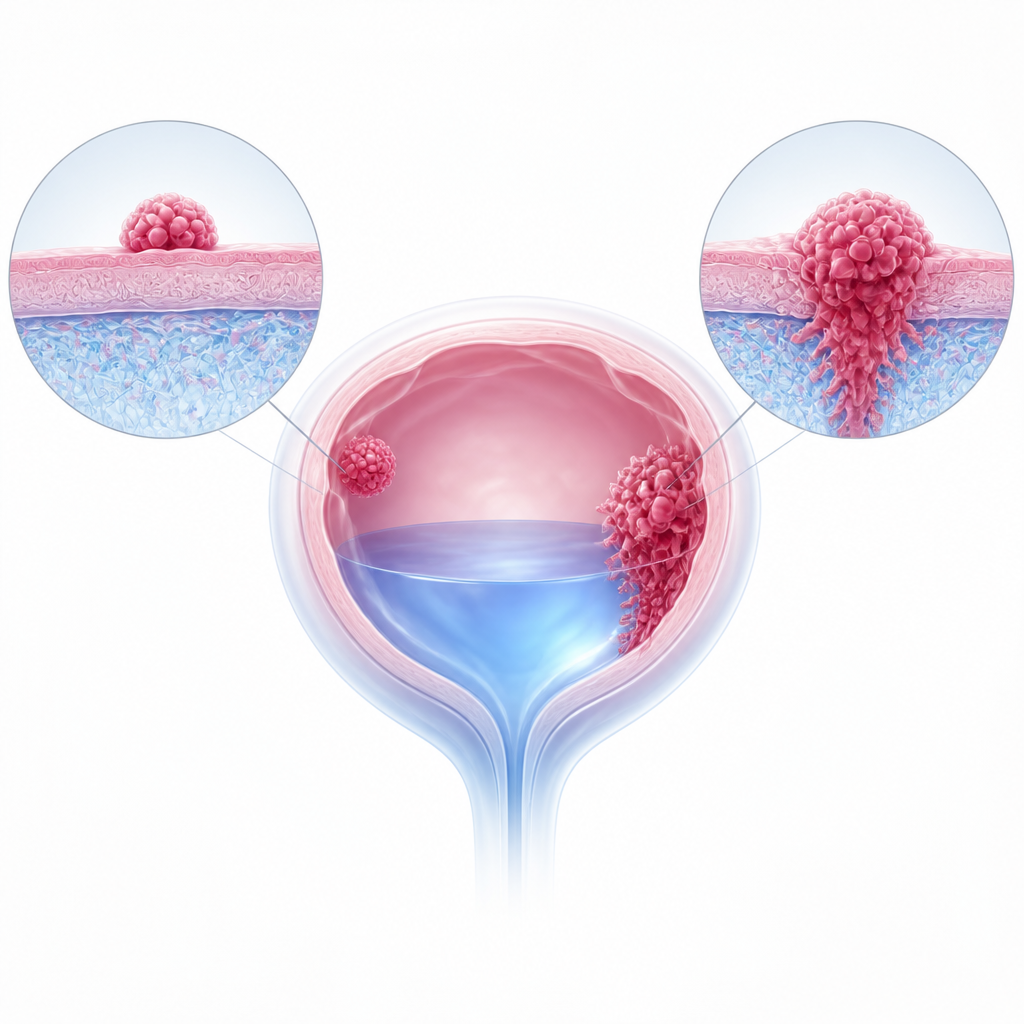
How Do Specialists Differentiate Non-Muscle-Invasive and Muscle-Invasive Bladder Cancer?
Bladder cancer is broadly categorized based on the depth of invasion. Urologists utilize transurethral resection of bladder tumor (TURBT) both as a primary diagnostic tool and a therapeutic intervention. According to the European Association of Urology (EAU) Guidelines (2022), approximately 75% of newly diagnosed bladder cancers are non-muscle-invasive. While NMIBC is confined to the mucosa or submucosa, it carries a high recurrence rate of up to 60-70% within five years. Conversely, Muscle-Invasive Bladder Cancer (MIBC) penetrates the detrusor muscle and requires aggressive treatments like radical cystectomy or systemic chemotherapy.
| Diagnostic Aspect | Non-Muscle-Invasive (NMIBC) | Muscle-Invasive (MIBC) |
|---|---|---|
| Invasion Depth | Confined to mucosa (Ta, Tis) or lamina propria (T1) | Penetrates detrusor muscle layer (T2 or deeper) |
| Primary Treatment | TURBT followed by intravesical therapy (BCG/Mitomycin-C) | Radical cystectomy, systemic chemotherapy, or radiation |
| Recurrence & Prognosis | High recurrence rate (up to 70%), but lower immediate mortality | High risk of systemic metastasis; requires intensive systemic therapy |
According to official guidelines from the American Urological Association (AUA) and clinical evidence, both quantitative grading systems and individual patient anatomy must be analyzed together to formulate a safe oncological strategy.
What Are the Key Diagnostic Protocols When Painless Hematuria Occurs?
The primary symptom of bladder cancer is gross hematuria, which is characterized by visible blood in the urine without any associated pain. This classic presentation often leads patients to delay consultation, assuming it is a simple urinary tract infection (UTI). However, multiple observational studies indicate that up to 20% of adults presenting with painless gross hematuria are eventually diagnosed with a urological malignancy. Advanced diagnostic modalities such as high-resolution cystoscopy, urinary cytology, and pelvic computed tomography (CT) urography are standard protocols in modern urology clinics in Ssangyong-dong. Identifying the cellular morphology early prevents disease progression. However, outcomes may differ in exceptional cases such as patients with chronic hemorrhagic cystitis or those undergoing anticoagulation therapy, where hematuria origin can be complex to trace.
- Routine urinalysis and urine culture: Conducted to exclude active infections or microscopic hematuria of renal origin.
- High-definition flexible cystoscopy: Visually inspects the bladder lining in real-time to locate any abnormal tissue growth.
- Urinary cytology: Analyzes cell morphology to detect high-grade malignant cells shed in urine.
- Multi-phase CT Urography: Evaluates the upper urinary tract (ureters and kidneys) to ensure no synchronous tumors exist.
- Biopsy or TURBT: Performed under anesthesia for definitive histopathological staging and grading.
- If a patient detects painless gross or microscopic hematuria,
- Then perform a complete urological workup including flexible cystoscopy and urinary cytology at a urology clinic in Ssangyong-dong…
- Then initiate customized TURBT or intravesical therapy based on the pathological stage and risk classification.
Frequently Asked Questions FAQ
QIs pain a common symptom of bladder cancer?
No, the hallmark sign of bladder cancer is painless hematuria. Pain during urination, frequency, or urgency typically suggests a urinary tract infection or bladder stones, but these can occasionally coexist with malignancy, necessitating professional evaluation.
QHow often does bladder cancer recur after surgical removal?
Non-muscle-invasive bladder cancer has a high recurrence rate, ranging between 50% and 70% depending on tumor grade and size. Because of this, regular follow-up cystoscopy and urine tests are mandatory every 3 to 6 months during the first few years post-treatment.
QWhat is intravesical therapy, and when is it used?
Intravesical therapy involves instilling liquid medication, such as Bacillus Calmette-Guérin (BCG) or chemotherapeutic agents, directly into the bladder via a catheter. It is standard practice after TURBT for intermediate to high-risk non-muscle-invasive bladder cancer to reduce recurrence rates.

This content is general medical information, and individual treatment decisions should be made through imaging tests and in-person medical evaluation.
Author: Medical content editor based on medical information research
Reviewed by: Specialist consultation from the relevant department
Last reviewed: 2026-06-22
Reference guideline: 2023 European Association of Urology (EAU) Guidelines on Non-muscle-invasive Bladder Cancer
Medical neutrality and closing note
The core of medical decision-making is not to follow a specific device or a trending procedure, but to choose an option that fits each patient’s individual anatomy, condition, risk level, and treatment goals. Every procedure has both advantages and limitations, so decisions should be made after sufficient discussion with an experienced specialist.
[Medical information and copyright notice]
This content is a professional medical column prepared based on medical consultation from 굿모닝비뇨기과.
The infographics used in this article are created to support understanding and may differ from actual clinical results.
The information provided is a general medical guideline, and accurate diagnosis and treatment require an in-person evaluation by a qualified specialist.