When is Urinary Stone Surgery Absolutely Necessary? Key Selection Guidelines at Ssangyong Station Urology
Why Do Urinary Stones Form, and When Do They Become a Medical Emergency?
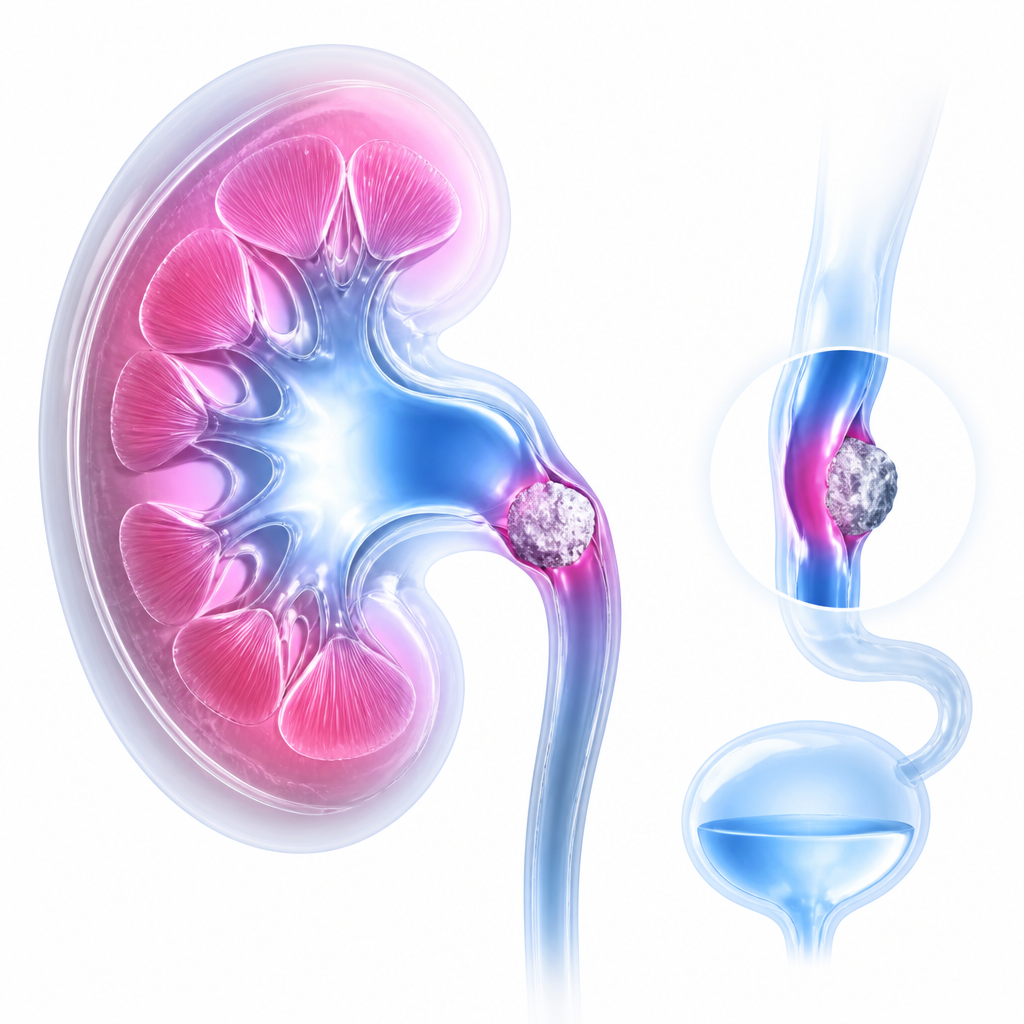
Urinary stone disease, or urolithiasis, is a progressive pathological condition characterized by the formation of crystalline mineral deposits within the renal pelvis, ureters, or urinary bladder, which can lead to complete mechanical obstruction of the urinary tract and subsequent hydronephrosis. When a stone blocks the flow of urine, pressure builds up in the kidney, leading to acute, excruciating flank pain known as renal colic. If left untreated, this severe mechanical obstruction can cause irreversible damage to renal function, potentially leading to renal atrophy or life-threatening systemic infections like pyelonephritis or urosepsis.
At Ssangyong Station urology clinics, specialists prioritize diagnostic accuracy to determine if the patient’s condition can be managed conservatively or requires immediate intervention. Factors such as stone size, location, degree of obstruction, and the presence of underlying infection dictate the urgency of the treatment. While small stones under 5mm often pass spontaneously with adequate hydration, larger or impacted stones require proactive surgical solutions to safeguard kidney health.
Treatment timing: Prompt surgery is indicated when the stone size exceeds 10mm, causes severe unmanageable renal colic, or presents with an active infection or complete tract obstruction.
Non-surgical care: Conservative management with high hydration and medical expulsive therapy is reasonable for asymptomatic stones under 5mm with no signs of hydronephrosis or infection.
Treatment selection: Choice of ESWL, RIRS, or PCNL depends on the stone size, anatomical location, and risk of renal damage, balanced with patient recovery expectations.
How Do Surgical Treatment Options Compare for Optimal Stone Clearance?
According to domestic and international clinical guidelines, including those published by the European Association of Urology (EAU) in 2023, the selection of surgical intervention depends on multiple quantitative criteria. The most common procedures include Extracorporeal Shockwave Lithotripsy (ESWL), Retrograde Intrarenal Surgery (RIRS), and Percutaneous Nephrolithotomy (PCNL). Each approach has distinct indications, benefits, and technical limitations that must be carefully balanced.
| Treatment Method | Recommended Stone Size | Key Advantage | Primary Limitation |
|---|---|---|---|
| ESWL (Shockwave Lithotripsy) | Less than 10 mm | Non-invasive, outpatient procedure with no anesthesia required. | Lower success rates for very hard stones or those in the lower pole of the kidney. |
| RIRS (Endoscopic Laser Surgery) | 10 mm to 20 mm | High stone-free rate, directly accesses the entire kidney via natural tracts. | Requires general anesthesia and the temporary placement of a ureteral stent. |
| PCNL (Percutaneous Surgery) | Greater than 20 mm | Highly effective for massive staghorn stones in a single session. | More invasive, requiring a small incision in the back and longer hospital stay. |
According to official clinical guidelines, both the absolute quantitative size of the stone and the patient’s individual anatomical variations must be evaluated together to optimize the stone-free recovery rate.

What Are the Key Diagnostic Criteria for Surgical Intervention?
Urological specialists evaluate specific clinical markers to determine whether a patient can continue conservative management or must undergo immediate surgery. A primary consideration is the presence of progressive hydronephrosis, which indicates that urine cannot bypass the stone, threatening renal parenchymal integrity. According to multiple observational studies and meta-analyses, delaying intervention for complete ureteral obstruction beyond 4 weeks significantly increases the risk of irreversible nephron loss.
Below is the checklist utilized by specialists to assess the necessity of surgical intervention:
- Unmanageable Pain: Renal colic that cannot be controlled with intravenous analgesics or oral medications.
- Active Infection: Presence of pyelonephritis, high fever, or systemic signs of urosepsis behind an obstructed kidney.
- Significant Size: Stone size exceeding 10mm, which has a less than 10% probability of spontaneous passage.
- Solitary Kidney or Bilateral Obstruction: Any obstruction in patients with a single functioning kidney requires emergency decompression.
- Failed Conservative Trial: No progress of stone movement after 4 to 6 weeks of medical expulsive therapy (MET) utilizing alpha-blockers.
To assist in patient decision-making, urologists use a structured algorithmic flow based on clinical presentation:
Step 1: If the stone is small (<5mm) with mild pain and no signs of infection or severe hydronephrosis, then pursue conservative management with medical expulsive therapy and high hydration for up to 4 weeks.
Step 2: If the stone size is between 5mm and 10mm, or if pain recurrences are frequent, then schedule elective ESWL or RIRS depending on stone location and hardness.
Step 3: If there is a complete obstruction, severe hydronephrosis, or a co-existing urinary tract infection with fever, then perform urgent endoscopic surgery (RIRS or stent placement) immediately to preserve renal function.
However, outcomes may differ in exceptional cases such as pregnant patients, patients with severe skeletal deformities, or those on irreversible anticoagulant therapy, where customized treatment protocols must be established.
Frequently Asked Questions FAQ
QIs urinary stone surgery painful, and what is the recovery time?
Modern endoscopic surgery (RIRS) is performed under general anesthesia, ensuring a pain-free procedure. Some postoperative discomfort or mild blood in the urine may occur due to the temporary double-J (DJ) stent, which typically resolves within a few days to a week after the stent is removed by a specialist.
QCan urinary stones recur even after a successful surgical removal?
Yes, the recurrence rate of urolithiasis is approximately 50% within 5 to 10 years without proactive preventive measures. Maintaining a daily urine volume of over 2.5 liters, reducing sodium and animal protein intake, and pursuing metabolic evaluation are critical to preventing recurrence.
QWhen should I immediately visit a urology clinic near Ssangyong Station?
You should immediately visit a specialized urology clinic near Ssangyong Station if you develop severe flank pain accompanied by a fever over 38°C, persistent chills, severe nausea, vomiting, or if you notice a complete cessation of urine flow.

This content is general medical information, and individual treatment decisions should be made through imaging tests and in-person medical evaluation.
Author: Medical content editor based on medical information research
Reviewed by: Specialist consultation from the relevant department
Last reviewed: 2026-06-17
Reference guideline: 2023 European Association of Urology (EAU) Guidelines on Urolithiasis
Medical neutrality and closing note
The core of medical decision-making is not to follow a specific device or a trending procedure, but to choose an option that fits each patient’s individual anatomy, condition, risk level, and treatment goals. Every procedure has both advantages and limitations, so decisions should be made after sufficient discussion with an experienced specialist.
[Medical information and copyright notice]
This content is a professional medical column prepared based on medical consultation from 굿모닝비뇨기과.
The infographics used in this article are created to support understanding and may differ from actual clinical results.
The information provided is a general medical guideline, and accurate diagnosis and treatment require an in-person evaluation by a qualified specialist.